Understanding ICD-10-CM Codes

In the world of healthcare, accurate coding is the backbone of efficient billing, reimbursement, and patient care management. One such critical coding system used across healthcare settings is the ICD-10-CM. The transition from ICD-9 to ICD-10-CM introduced a more detailed coding system, enabling healthcare providers to document diagnoses with greater specificity. This enhanced granularity has led to improved documentation accuracy, which is essential for precise diagnosis and treatment planning.
A study by the AHIMA Foundation found that adopting ICD-10-CM has improved clinical coding accuracy. A review of over 30,000 records after ICD-10 implementation showed that 38% of respondents noticed changes in coding accuracy, with some reporting significant improvements. In this blog, we will explore ICD-10-CM codes, their structure, uses, and how they can help ensure better healthcare outcomes.
What Are ICD-10-CM Codes?
ICD-10-CM (International Classification of Diseases, 10th Revision, Clinical Modification) is a standardized system used to classify and code all diagnoses, symptoms, and procedures recorded in conjunction with hospital care. Developed by the World Health Organization (WHO) and adapted for use by the National Center for Health Statistics (NCHS) in the U.S., ICD-10-CM provides an essential framework for diagnosing and documenting diseases, conditions, and reasons for visits across all healthcare settings.
ICD-10-CM Structure Format
ICD-10-CM codes are alphanumeric, consisting of up to seven characters, and have a structured format designed to provide detailed and specific information about diseases, conditions, and diagnoses. Understanding the format is crucial for accurate coding and appropriate billing. Here’s a breakdown of the structure:
Character Length
ICD-10-CM codes range from 3 to 7 characters long, with each character providing essential information about the diagnosis.
- 3-Character Codes: The shortest codes in ICD-10-CM, such as P09, are typically used for simple conditions or when the full specificity isn’t needed.
- Codes Longer than 3 Characters: These codes include a decimal point after the first three characters, such as S32.010A or O9A.211, and provide more detailed information about the condition, including severity, location, and the patient's condition. The decimal is placed after the first three characters to separate the general category from the more specific details.
Character Composition
- 1st Character: The first character is always an alphabetical letter, representing the chapter or category of the condition.
- 2nd to 7th Characters: These can either be alpha or numeric. These additional characters offer more detailed information, such as the type of condition, the location of the condition, or the severity.
7th Character
The 7th character is used in specific chapters, such as obstetrics, musculoskeletal disorders, injuries, and external causes of injury. For instance, a code like M1A.0111 (which refers to osteoarthritis) uses the 7th character to indicate the specific stage or complexity of the condition.
By following this structured approach, ICD-10-CM codes allow for accurate diagnosis classification, ensuring consistency and precision across the healthcare system.
Benefits of ICD-10-CM

The adoption of ICD-10-CM (International Classification of Diseases, 10th Revision, Clinical Modification) has ushered in significant enhancements across various facets of healthcare. Its comprehensive and detailed coding structure offers numerous benefits, including:
- Enhanced Data Quality: ICD-10-CM provides more precise data for measuring the quality, safety, and efficacy of care, facilitating better assessment and improvement of healthcare services.
- Improved Reimbursement Processes: The specificity of ICD-10-CM codes aids in designing payment systems and processing claims for reimbursement, ensuring that healthcare providers receive appropriate compensation for the services they deliver.
- Advanced Research Capabilities: With its detailed classification, ICD-10-CM supports conducting research, epidemiological studies, and clinical trials, contributing to the advancement of medical knowledge.
- Informed Health Policy Development: The granular data captured through ICD-10-CM codes assist in setting health policies by providing insights into disease patterns and healthcare needs.
- Strategic Healthcare Planning: Operational and strategic planning, including the design of healthcare delivery systems, benefits from the comprehensive data provided by ICD-10-CM, leading to more effective healthcare services.
- Efficient Resource Utilization Monitoring: ICD-10-CM enables the monitoring of resource utilization, helping in the optimal allocation of healthcare resources.
- Enhanced Performance Improvement: The detailed information from ICD-10-CM codes contributes to improving clinical, financial, and administrative performance within healthcare organizations.
- Fraud and Abuse Detection: The specificity of ICD-10-CM codes aids in preventing and detecting healthcare fraud and abuse by identifying inconsistencies and anomalies in coding.
- Public Health Surveillance: ICD-10-CM plays a crucial role in tracking public health trends and risks, facilitating timely responses to health emergencies.
Incorporating ICD-10-CM codes into healthcare practices significantly contributes to the overall improvement of patient care and public health outcomes.
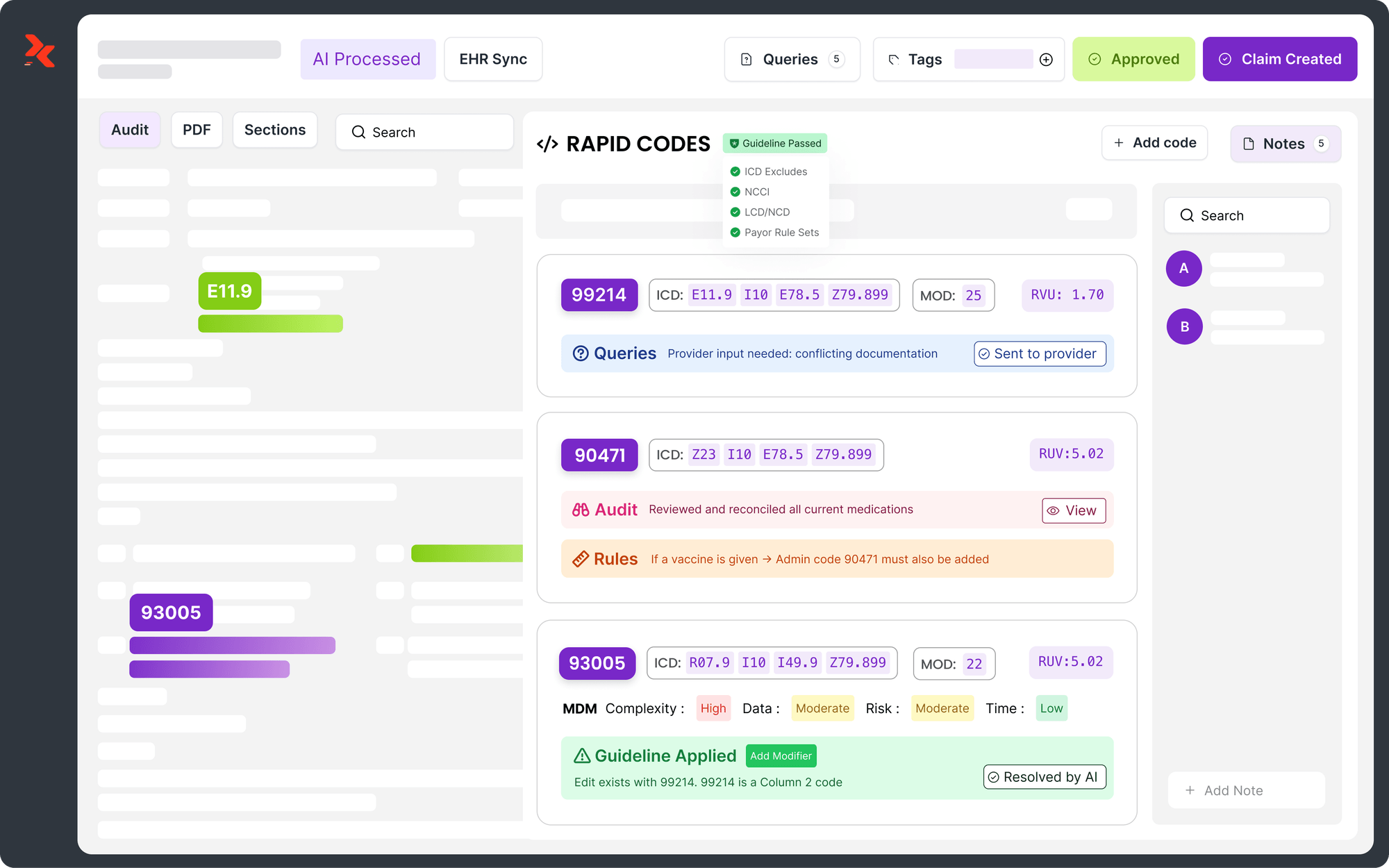
To further enhance the benefits of ICD-10-CM adoption, RapidClaims’ coding modules offer cutting-edge solutions designed to streamline and optimize the coding process. Their services include Hierarchical Code Analysis across over 90,000 codes, integration of Social Determinants of Health (SDOH) Coding, and 7th-digit precision for optimal accuracy. Additionally, RapidClaims provides automated updates of new ICD official guidelines and rare disease detection, ensuring that healthcare organizations remain compliant and efficient while reducing errors in the coding and reimbursement process.
The Shift from ICD-9-CM to ICD-10-CM
The transition from ICD-9-CM to ICD-10-CM marked a pivotal moment in healthcare coding. This change, implemented on October 1, 2015, was driven by the inadequacies of ICD-9-CM in accurately reflecting the complexity of contemporary medical diagnoses. ICD-10-CM offers a broader and more detailed code set, meeting the growing demands for precise data management, reporting, and analysis in the healthcare sector.
ICD-10-CM Official Guidelines

The official guidelines for ICD-10-CM provide clear instructions for coders to follow, ensuring consistency and accuracy in the coding process. These guidelines, updated annually, help coders understand how to correctly use codes in various clinical and administrative contexts. Let’s break down the key points that will guide you through using ICD-10-CM effectively.
1. Understand the Structure of ICD-10-CM Codes
ICD-10-CM codes are made up of 3 to 7 characters, each with a specific function. The first character is always a letter, and the remaining characters can be numbers or letters, depending on the level of specificity required. For example, R10.13 represents "Epigastric pain," with R being the chapter, 10 defining the symptom, and the last characters identifying the specific condition.
2. Collect Comprehensive Patient Data
Before assigning codes, it's crucial to gather all relevant information from the patient's visit, including:
- The patient's medical history and clinical records
- Specific details about the diagnosed condition
- Any pertinent lab results or imaging findings
3. Use the Alphabetic Index and Tabular List
To find the correct code, coders first reference the Alphabetic Index of ICD-10-CM, which helps them find the condition by its name. Once the main term is found, the coder uses the Tabular List to confirm the code’s full description and check for additional instructions such as the use of laterality, severity, or required secondary codes.
- Alphabetic Index: It is a list of conditions sorted alphabetically to find the related code.
- Tabular List: Once the code is found in the Alphabetic Index, it’s necessary to verify it by reviewing the full description in the Tabular List to ensure it applies to the patient's condition.
4. Follow Specific Coding Guidelines
Each year, CMS and the NCHS provide updated guidelines to clarify how ICD-10-CM should be used. Some of the key guidelines include:
- Level of Detail: Diagnosis codes should be used at the highest level of specificity. For example, if a code can be subdivided further into more detailed codes, the more detailed version should be used.
- Symptoms and Signs: Symptoms should be coded when no definitive diagnosis is available. However, the presence of a symptom code does not preclude using a diagnosis code once it is confirmed by the physician.
- Multiple Coding: Some conditions require more than one code to fully describe the diagnosis. For example, bacterial infections may require a code for the infection itself, along with a code to identify the specific bacteria causing it.
5. Use of Combination Codes
A combination code is a single code used to classify two diagnoses or a diagnosis with an associated secondary process or complication. For example, a code for diabetes with a complication, such as E11.9 (Type 2 Diabetes Mellitus), might also include the associated condition in one combination code. Coders should use a combination code whenever it fully captures the complete diagnostic picture. If it does not, a secondary code should be used.
6. Acute and Chronic Conditions
In cases where the same condition is described as both acute and chronic, coders should assign both codes. The acute condition should be sequenced first when both are present. For example, a patient might have acute bronchitis as well as chronic bronchitis, and both conditions should be coded accordingly.
7. Sequela (Late Effects)
Sequela refers to the residual effects after an injury or illness has resolved, which may manifest immediately or after a long period. When coding for sequela, use two codes: the condition causing the sequela first, followed by the sequela code. In some cases, the sequela code may include the manifestation at the 4th, 5th, or 6th character level, or a manifestation code may follow. There is no time limit for sequela, as it can appear months or even years later, such as infertility from past tuberculosis or scarring from burns.
8. Documentation and Compliance
Thorough documentation is critical for accurate coding. Every ICD-10-CM code selected must be supported by clear and sufficient clinical documentation from the healthcare provider. If a diagnosis is ambiguous or the clinical documentation doesn’t match the selected code, the coder should seek clarification from the provider.
9. Regular Updates and Payer-Specific Requirements
ICD-10-CM coding guidelines are regularly updated to ensure compliance with the latest healthcare regulations and payer requirements. Insurance payers may have specific rules or guidelines that must be followed, so it is essential to stay updated on any changes and confirm that the coding practices align with the payer's policies.
These guidelines ensure that healthcare providers are reimbursed appropriately for the services they provide while also improving the quality of care and maintaining compliance with industry standards.
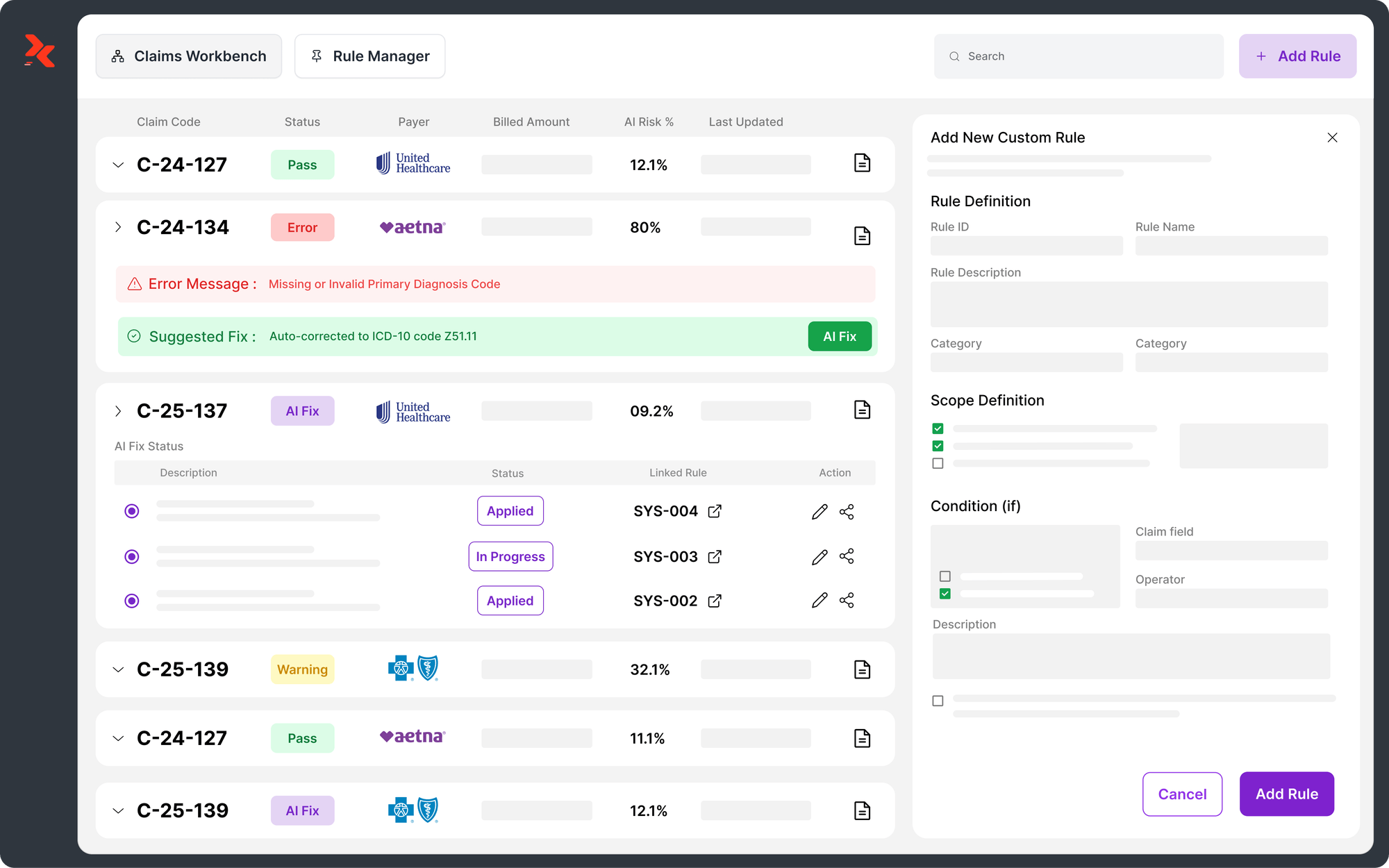
After thoroughly understanding and applying the ICD-10-CM official guidelines, it’s essential to ensure your coding process remains accurate and compliant. RapidClaims’ suite of AI-powered solutions can help streamline this process, providing real-time updates and automated suggestions that ensure adherence to the latest ICD-10-CM guidelines. With tools like RapidCode, RapidAssist, and RapidRisk, healthcare providers can significantly reduce coding errors and improve their reimbursement accuracy.
Using the ICD-10-CM Tabular List
The ICD-10-CM Tabular List is essential for accurate coding and organizing codes systematically by numerical value. It includes instructional notations like Includes, Excludes1, Excludes2, and Code First/Use Additional Code, guiding coders in selecting the correct codes. These notes provide definitions and instructions for applying codes in specific scenarios.
1. Includes
The word "Includes" appears immediately under certain categories in the ICD-10-CM system to clarify and further define the content of that category. It provides examples or additional details to ensure that coders understand which specific conditions or diagnoses fall under a particular code. The Includes note ensures that coders don't mistakenly overlook conditions that are related to a certain diagnosis.
2. Excludes Notes
ICD-10-CM features two types of Excludes notes to help coders identify which conditions cannot be grouped under the same code. These notes are particularly useful when there are exceptions in coding, ensuring accurate and precise categorization.
3. Excludes1
An Excludes1 note means “NOT CODED HERE!” This is a strict rule that indicates two conditions cannot be coded together. These conditions are mutually exclusive and cannot occur simultaneously in the same patient. An Excludes1 note is typically used when one condition contradicts the other, such as when a congenital form of a condition cannot coexist with an acquired version of the same condition.
4. Excludes2
The Excludes2 note, on the other hand, indicates that the condition excluded is not included here, but it can be coded together with the primary condition. These exclusions are used when two conditions are related but distinct from one another, meaning they don't belong together under one code but could occur simultaneously.
For example, the Tabular List entry for R18 (Ascites) shows how conditions are described in detail:
R18 Ascites
- Includes: Fluid in the peritoneal cavity
- Excludes1: Conditions like ascites due to alcoholic cirrhosis (K70.31), alcoholic hepatitis (K70.11), and others.
This structure ensures clarity and consistency when selecting the correct code.
5. Code First / Use Additional Code
The "Code First" note directs coders to report the underlying condition before its manifestations. For example, if diabetes causes complications like neuropathy, code diabetes first, then the complication. The "Use Additional Code" note indicates that an extra code is required to fully describe the condition, with the order depending on severity or reason for the encounter.
6. 7th Characters and Placeholder "X"
Some codes require a 7th character for additional specificity, such as indicating the stage or encounter type. If the code is less than six characters, the "X" placeholder is used to ensure proper length. For example, "M17.11" identifies "unilateral primary osteoarthritis, right knee" in the acute stage, with the 7th character distinguishing subsequent care or long-term effects.
With a clear understanding of how the ICD-10-CM Tabular List functions, let's explore the most recent 2025 updates that impact how these rules are applied.
ICD-10-CM Updates
The April 1, 2025, update to the ICD-10-CM system introduced several important changes, although no new diagnosis codes were added. Instead, the updates focused on revisions, deletions, and additions to various sections of the coding system, including the Index to Diseases and Injuries, the Tabular List, and the Official Guidelines for Coding and Reporting.
Here is a breakdown of the updates made in the April 2025 release:
Updates to the Index to Diseases and Injuries
- One code deleted: A specific code has been removed from the Index.
- Three codes replaced: Some existing codes were substituted with new ones for better accuracy or classification.
- Three subterms moved: These subterms were shifted to a further level of indentation to improve clarity in the indexing structure.
- One spelling correction: A few entries were corrected for spelling, ensuring consistency across the system.
Changes in the Tabular List of Diseases and Injuries
- One change to subcategory instructions: The guidelines for certain subcategories have been updated to enhance clarity.
- Excludes1 and Excludes2 Notes:
- One Excludes1 note added: A new restriction has been introduced, specifying that certain conditions cannot be coded together.
- One Excludes1 note deleted: A previous restriction has been removed, allowing for more flexibility in coding.
- One Excludes1 note changed to an Excludes2 note: This change allows for the concurrent coding of previously excluded conditions under specific circumstances.
- One change to an Excludes2 note: Adjustments were made to allow for clearer coding guidelines.
- Instructional Notes:
- Seven new instructional notes were added to provide further guidance for coders.
- One existing instructional note was revised to clarify coding instructions.
- One spelling correction was applied to improve consistency and accuracy.
Updates to the Official Guidelines for Coding and Reporting
- Changes to guideline I.C.1.g.1.h: A minor change was made to refine existing coding instructions.
- Introduction of new guideline I.C.4.b.1: A new guideline was added to offer more specific guidance on certain coding practices.
Other Sections
- Table of Neoplasms: No updates were made to the Neoplasm table.
- Table of Drugs and Chemicals: No changes were implemented in the drug classification table.
- External Cause of Injuries Index: No revisions were made to this index.
These updates ensure that ICD-10-CM continues to reflect the evolving nature of medical practice and diagnoses. The changes provide coders with clearer guidelines and ensure that the system remains effective in tracking health conditions and facilitating accurate reimbursement. Understanding these updates is crucial for healthcare providers to stay compliant and ensure the accuracy of their billing and documentation practices.
RapidClaims helps healthcare providers stay aligned with the latest ICD-10-CM updates by offering automated updates that incorporate new coding changes as soon as they’re introduced. With RapidClaims, users can quickly adapt to the latest revisions and updates, ensuring compliance and minimizing the risk of coding errors.
Conclusion
ICD-10-CM coding is essential for accurately documenting diagnoses, improving billing accuracy, and supporting public health efforts. Its detailed structure enhances healthcare providers' ability to capture a wide range of conditions with greater specificity, driving better patient outcomes, reducing financial risks, and ensuring appropriate reimbursement. The transition from ICD-9 to ICD-10-CM allowed for a much more precise and comprehensive system, enabling providers to better navigate the complexities of modern healthcare.
At RapidClaims, we understand the challenges of staying updated with ICD-10-CM guidelines. Our AI-driven solutions—RapidCode, RapidAssist, and RapidRisk—help simplify coding processes, ensure accurate billing, and optimize revenue cycle management. With real-time updates and automated coding recommendations, we ensure your organization remains compliant and efficient.
Ready to simplify your coding process and boost your compliance? Contact RapidClaims today to see how our innovative solutions can transform your medical coding and improve reimbursement accuracy.
Frequently Asked Questions (FAQs)
1. What is ICD-10-CM used for?
ICD-10-CM codes classify and document diagnoses and procedures in healthcare, ensuring accurate billing, reimbursement, and disease tracking.
2. How does ICD-10-CM differ from ICD-9-CM?
ICD-10-CM provides more detailed and specific codes, capturing the complexity of modern diagnoses that ICD-9-CM couldn’t, improving patient care and reimbursement.
3. How do ICD-10-CM updates affect coding and reimbursement?
ICD-10-CM updates refine codes and guidelines, ensuring accurate documentation and reimbursement, and helping providers stay compliant with evolving medical practices.
4. What are Excludes1 and Excludes2 in ICD-10-CM?
"Excludes1" means two conditions cannot be coded together, while "Excludes2" means they can occur together but must be coded separately.
5. How can RapidClaims assist with ICD-10-CM coding?
RapidClaims offers AI-powered tools like RapidCode, RapidAssist, and RapidRisk, ensuring accurate, compliant coding with real-time updates and automated suggestions.

Team RapidClaims
Latest Post
expert insights with our carefully curated weekly updates
Related Post



Top Products